Development of Affordable and Reliable Diagnostic Tools to Record Vital Parameters for Improving Health Care in Low Resources Settings
Mannan Mridha, Usama Gazay, Kosovare V. Aslani, Hugo Linder, Alice Ravizza and Carmelo de Maria
Abstract—In most developing countries, although the vast majority of the people are living in the rural areas, the qualified medical doctors are not available there. Health care workers and paramedics, called village doctors, informal healthcare providers, are largely responsible for the rural medical care. Mishaps due to wrong diagnosis and inappropriate medication have been causing serious suffering that is preventable. While innovators have created many devices, the vast majority of these technologies do not find applications to address the needs and conditions in low-resource settings. The primary motive is to address the acute lack of affordable medical technologies for the poor people in low-resource settings. A low cost smart medical device that is portable, battery operated and can be used at any point of care has been developed to detect breathing rate, ECG and arterial pulse rate to improve diagnosis and monitoring of patients and thus improve care and safety. This simple and easy to use smart medical device can be used, managed and maintained effectively and safely by any health worker with some training. In order to empower the health workers and village doctors, our device is being further developed to integrate with ICT tools like smart phones and connect to the medical experts wherever available, to manage the serious health problems.
Keywords—Healthcare for low resources settings, health awareness education, Improve patient care and safety, Smart and affordable medical device.
I. INTRODUCTION
In most developing countries, qualified medical doctors are not available in the rural areas. Lack of pure drinking water, lack of proper sanitation system, air pollution, malnutrition, protein deficiency and food contamination are the primary causes of illnesses in the low resources settings. Lack of health awareness education, regular income, and proper life style management further deteriorates their health conditions. Rural health care facilities in the developing countries usually do not have qualified health staff and healthcare equipment to offer reliable healthcare access to those who need it most. Current health care delivery system needs an urgent improvement to make it accessible, affordable, equitable and safe as well as to make it fit-for future need. A more balanced workforce that is applicable to each country’s needs and conditions is required. Appropriate education, training and incentives should be focused on creating an efficient workforce that is centered on disease prevention as well as illness management, which will be able to function with coordinated action [1,2].
There severe shortage of healthcare workers in most developing countrie. Africa has 2.3 healthcare workers per 1000 population, compared with the Americas. In low-resource settings, like rural India or Bangladesh, 70% of the country’s population lives in the rural areas, and they do not have adequate access to health care. Almost 76% of the country’s medical facilities are concentrated in the urban areas.Infact there is an overall shortage of medical personnel in the country. Medical devices are generally unavailable, underutilized or misused [3,4] at the government health care facilities. This is largely due to shortages of biomedical engineers, clinical engineering facilities at the hospitals, and lack management and maintenance services along with the shortages of spare parts and proper education and training materials.
Cardiovascular disease causes thirty-two percent of all deaths and eighty percent of which occur in low- to mid-income countries. By 2020, cardiovascular diseases are predicted to be the major causes of morbidity and mortality in most developing nations around the world [5]. Respiratory and pulmonary infections, influenza, heart diseases etc. pose major public health-related complications in Bangladesh with consequent high morbidity and mortality [4]. By enabling remote telemedicine diagnostics, the smartphone-powered devices can connect patients living in rural areas with cardiologists and other experts, and can enable physicians to make better decisions, leading to better outcomes [6,7].
The main purpose of this work is to address the lack of reliable and affordable medical technologies in low-resource settings to monitor Pulmonary and Cardiovascular diseases that represent a leading cause of mortality and morbidity especially among the elder people and manage illness of the infants. It is also important to create an enabling environment to improve the rural health workers’ quality and performance through access to:
a) reliable and cost effective medical devices for quality diagnosis,
b) proper education and training to manage the related devices and ICT tools,
c) reliable connectivity to the medical experts for consultation and treatment advice
d) education to prevent and treat health problems which routinely afflict the rural people.
II. DESIGN AND DEVELOPMENT
Innovative medical technologies offer more effective medical care, with less risk to patient and healthcare personnel. Medical technology and device must play important role in developing regions too, because better data, more accurate diagnosis and monitoring can improve patient care and safety among the rural marginalized and disadvantaged group of population. Quality treatment can lead to less invasive treatments and can be more targeted and often less costly [8]. Remote health monitoring using noninvasive sensors and modern communication technologies offers an efficient and cost-effective solution increasing the accessibility, acceptability, adaptability, affordability and availability of high quality assistive devices and medical devices. This will also allow healthcare personnel to monitor important physiological signs of their patients in real time, assess health conditions and provide feedback from distant facilities. In this work, we have developed low-cost, smart and non-invasive monitoring system to monitor arterial pulse rates using Optical and Piezoelectric sensors. A handheld, safe and user friendly heart rate monitor has been developed using smart and low cost sensors and easily available cost effective electronic components and microcontroller. The device consists of two modules. First, low cost smart and sensitive multiple sensors (Piezo, Optical, Thermal and ECG electrodes) interfaced with smart circuits including capacitors, resistors and instrumentation amplifiers, INA 128. The circuits are developed
Fig. 1 shows the Optosensor, Piezoelectric sensor and Thermistor sensors fitted in the houses for recording.
Fig. 2 The TCRT1000 are a reflective Optosensors which include an infrared emitter and phototransistor in a leaded package which blocks visible light.
Second, the analog output signal from the sensors are filtered and amplified to improve Signal Noise Ratio. The analog signal is processed by a microcontroller to provide significant information about the patient’s breathing rate, heart rate and ECG. The display device present the graphcal representation of the heart lung function as well as present irregularity in the heart or breathing activity if any.
When an index finger is placed on the optosensor, the light from the photodiode is reflected from the red blood cells and detected by the phototransistor housed in the same sensor. The output signal from the opto sensor contains a large dc voltage with a tiny dynamic signal. Therefore, it is required to use a high pass filter with a cut off frequency as low as a few Hertz to get rid of the dc component. Later, the signal is amplified using an instrumentation amplifier INA128.
Fig. 3 shows how the Themistor is connected to Wheatstone Bridge and Instrumentation amplifier record the breathing rate.
The signal is further filtered to improve Signal to Noise Ratio. A piezoelectric sensor is used to record arterial pulse pressure from the radial artery near the wrist. Breathing rate was obtained by using a sensitive Thermistor connected to a Wheatstone bridge and Amplifiers. The display shows the breathing activity, ease of breathing or high resistance to breathing can be observed from the slope of the curve. In case of patients with breathing difficulties, treament effectiveness can be observed from the curves.
Fig. 4 shows the ECG recording circuit with amplifier and Band pass active filter. (RA = Right Arm, LA= Left Arm and RL= Right Leg).
ECG was recorded with three lead connections using electrodes as sensors and the Instrumentation Amplifiers type INA 128, and active bandpass filter. The device is suitable for health workers to carry to the point of care to obtain consultation with the experts’ physicians. The ECG device technology is a low-cost portable one that can allow medical professionals to acquire ECG readings of patients with symptoms of cardiovascular disease from rural or remote areas who do not have physical access to qualified medical care.
Fig. 6 shows unprocessed and processed signal recording of arterial pulse pressure rate from optosensor when the fingertip was placed on the sensor. Certain Irregular betas are observed.
III. TEST RESULTS
Results from the tests in the lab performed on students show reproduceble and high quality output signal from the sensors. The signals can be processed to obtain the average data like breathing rate, interval between breaths, and heart rate and interval between beats on a display. Measurement system allows choosing one sensor type at a time. Following digitization of the analogue signal, a pulse amplitude–time graph and relevant statistical parameter to detcet the irregularies are displayed on an LCD screen that presents multiple sensor values. The values can be used for monitoring purpose and can provide guidelines for recommendation for through diagnostic tests. This battery powered, electrically safe and cost effective diagnostic device has been tested on both adults and children, and the results have been found to be accurate, reliable and reproducible.
Fig. 6 Typical recordings from thermistor indicating breathing rate, and the inhalation and exhalation activity are traced from the slope of the increase and deccrease of the curves.
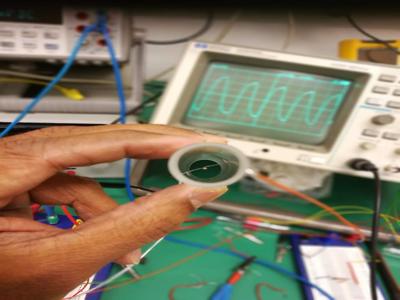
Fig. 7 Typical recordings from ECG Electrodes shown on the oscilloscop. The same can be obtained on laptop, or microcontroller or smart phone dispaly for sending to the medical expert.
İt is a committment of this Project to provide safe and reliable medical devices. For this reason the safety profile of the device shall be analysed according to the internationally recognised standard on risk management ISO 14971. The preferred methods to ensure patient safety are methods based on design solutions (safe-by-design). Risk minimisation is ensured by desing for compliance to internationally recognized standard IEC 60601-1 that provides requirements on protection of both the patient and the operatör against electrical and mechanical hazards. Moreover, collateral and additional standards for Electromagnetic compatibility (IEC 60601-1-2), usability and alarms for human error prevention (IEC 60601-1-6, IEC 60601-1-8 and ISO 62366) and biocompatibility of parts in direct contact with the patient’s skin (ISO 10993) will be taken into account to provide safe-by-design solutions. Device reliability in terms of data processing may be ensured by application of IEC 62304 to the management of the Software lifecycle and testing, taking into account that the embedded Software can be classified as A, according to said standard. Further Project development may include testing for compliance of the aforementioned standards and for compliance to product-specific standards such as for example IEC 60601-2-25 for the ECG modüle. If this product would be commercially manufactured and placed in the market in Europe, it would be classified as a class IIa medical devices, active, for monitoring purposes in non-emergency situations.
Test reports would then be integrated in a full product technical file to ensure compliance to Essential Requirements of the current (2018) European Directives and the upcoming European Regulation (2020). Additional requirements would also have to be met, in order to ensure a consistent level of quality of the manufactured product and to ensure compliance to surveillance and vigilance regulatory requirements in the post market phase.
IV. DISCUSSIONS
Today, in all countries, we find the rapid increase of ageing population with fewer younger people to look after the elderly. We beleive that information and communication technologies will play a vital role in the provision and delivery of health care. e-health technologies enable remote patient monitoring; better dissemination of information to patients; improved access to health advice; access to remote consultations and telemedicine and quicker access to emergency services. According to WHO, e-health technologies has potential to help to improve training for health-care workers. With increased comptetnce and capacity and accountabilty, the health workers will be well able to manage disease surveillance, data collection and the management of patient records in a transparent. All these will increase patient care, and patient safety [9,10].
At present, the interpretation of sensor readings is focused towards determining the Heart rate, ECG and Breathing rate and Breathing functional characteristics. This battery operated, low cost handheld device is being further developed to provide more relevant vital parameters by integrating additional sensors for example, to determine Oxygen Saturation, Blood Pressure and Body Temperature to provide medical data that the health workers can report to the medical doctor for quality treatment guidelines. The sensors systems are under further development process to store, process and develop smooth communicate between health workers at different ends through smart phone for necessary interventions. We plan in our work to include Smartphone that is already widely used in healthcare, and has more potential to promote global interaction, improve care and reduce healthcare costs [6-8]. It is clear that the mobile phone is the vehicle for reaching the underserved with interventions from health and other sectors of the economy. Rural population in the developing world should benefit from such devices. With access to electricity and Internet this kind of medical devices together with cell phone-enabled application can empower the rural health workers to provide better and safer care. Thus the rural health workers working in poorly resourced settings are able to deliver quality diagnosis and care through access to real-time support by a doctor or specialist at a remote location. This functionality increases the use of medical experts for the citizens living in the rural areas in the developing world. Future challenges are expected in making the application available to the general population for home health applications for up-scaling the solution and making accessible to a wider audience in various settings. Some self-use education materials, electronic user manuals and video demonstrations need to be developed in local languages for family members and individual users for applications in at home or any level of healthcare centre. This kind of cost effective device contributes to the growth of eHealth that has the potential to resolve health disparities, and as a result, lead to health justice as described elsewhere [11].
V. CONCLUSIONS
This simple battery operated smart device can be used at any point of care to detect breathing and ECG along with arterial pulse rate to improve diagnostic care and patient safety. As a sustainable approach, we develop affordable medical devices for empowering health workers and village doctors and train them to use the devices and appropriate ICT tools, and connect them to the medical experts wherever available to manage the health problems and thus utilise the unique potential of mobile technologies to reduce disparities because of their extensive use in communities. These devices can improve their performance, increase their income, improve their social dignity and can provide the incentives that improve productivity, patient satisfaction and performance.
Acknowledgement
This project has received funding from the European Union’s Horizon 2020 research and innovation programme under Grant Agreement No 731053, UBORA.
References:
[1] Mumbo Hazel Miseda et al. The implication of the shortage of health workforce specialist on universal health coverage in Kenya, Hum Resour Health. 2017; 15: 80.Published online 2017
[2] Right to Healthcare around the Globe. Right to healthcare situation for children worldwide. https://www.humanium.org/en/right-to-health/
[3] World Health Organization. Children: reducing mortality. http://www.who.int/mediacentre/factsheets/fs178/en/.
[4] WHO compendium of innovative health technologies for low resource settings, http://www.who.int/medical_devices/innovation/compendium/en/
[5] V Bhatt, S Giri and S Koiral (2008). Health workforce shortage: a global crisis. The Internet Journal of World Health and Societal Politics Volume 7 Number 1. http://ispub.com/IJWH/7/1/6202
[6] WHO. (2014). Call for innovative health technologies for low-resource settings. Retrieved from http://www.who.int/medical_devices/innovation/call_2014/en/.
[7] Thairu L et al., Innovative newborn health technology for resource-limited environments. TropMedIntHealth. Vol 18(1): 117-128, 2013.
[8] Jonathan Mayes, Andrew White http://www.ghjournal.org/how-smartphone-technology-is-changing-healthcare-in-developing-countries/
[9] http://www.who.int/bulletin/volumes/90/5/12-040512/en/
[10] https://www.ncbi.nlm.nih.gov/books/NBK373436/
[11] Hamid Moghaddasi PhD, Masoud Amanzadeh MSc, Forough Rahimi PhD, Mahnaz Hamedan MSc, eHEALTH EQUITY: CURRENT PERSPECTIVES, http://journals.ukzn.ac.za/index.php/JISfTeH/article/view/170/792
Mannan Mridha, Usama Gazay and Kosovare Valle Aslani and Hugo Linder are with the Department of Biomedical Engineering, KTH The Royal Institute of Technology, Stockholm, Sweden (e-mail: mannan@kth.se).
Alice Ravizza and Carmelo De Maria is with the Research Center "E. Piaggio" - University of Pisa, Largo Lucio Lazzarino 1, 56122 Pisa, Italy.